


EVALUATION OF QUALITY OF LIFE IN PATIENTS WHO HAVE UNDERGONE SURGICAL TREATMENT FOR IDIOPATHIC SCOLIOSIS
Abstract
Objective: To evaluate quality of life via SF-36 questionnaire, in patients with Adolescent Idiopathic Scoliosis (AIS) who have undergone surgery for deformity correction, comparing the results at pre- and postoperative periods. Methods: We evaluated 29 patients, 24 females, with a mean age of 14.5 years old, all of them presenting measures of the Cobb angle greater than 50º and replied to the SF-36 questionnaire at the preoperative period and two years after surgery, on average. Results: We observed improvement in all eight components assessed by SF-36 after surgical treatment, with statistically significant improvement in the following components: physical functioning, role-physical, bodily pain and general health. Vitality and mental health presented the lowest percentage of improvement postoperatively. Conclusion: Surgical treatment for deformity in AIS improved the functional aspects assessed by the SF-36, representing, in practice, an improvement in the quality of life of these patients. Evidence Level II, prospective study. Keywords Scoliosis; Quality of Life; Treatment Results *Corresponding author Email: th.cmaia@gmail.com
Introduction
Idiopathic scoliosis is the lateral deviation of the spinal cord frontal plane larger than 10 degrees, without any described cause, which affects about 2-3% of the general population, being more prevalent in female teenagers. The most frequent complaint is due to aesthetical issues and, less frequently, pain, paresthesia, sphincter disorders or loss of body balance that may occur.1,2 Although the etiology of idiopathic scoliosis remains unknown, there are several different multifactorial hypotheses, such as neuromuscular or connective tissue alterations, hereditary factors, alterations in the sagittal configuration of the spinal cord, asymmetric growth of limbs and torso, besides environmental factors, such as nourishment.3-6 Studies show non-treated scoliosis results in higher incidence of pain and disablement, which may lead to work-related and marital problems, besides causing respiratory dysfunction and even early death.7-9 For those severe cases, the orthopedist is responsible for referring patients to surgical treatment in order to prevent the progression of the condition, correct the curve and keep the spinal cord balance.10 However, even with proper treatment, it is known that there is a significant decrease in quality of life in patients who suffer from severe deformities, affecting daily activities common to teenagers, as well as their psychosocial development.11 The term ‘quality of life’ has been used in the healthcare milieu since 1970 and comprehends a multidimensional concept, capturing the general health status impact, including disease and treatment in their physical, psychological and social aspects. Usually, the quality of life in a healthcare context is assessed through questionnaires due to the fact they allow higher reliability in treatment evaluation, being capable of revealing both positive and negative interferences in the patients’ lives. When we analyzed quality of life in patients with Adolescent Idiopathic Scoliosis (AIS) at pre- and postoperative periods via SF-36 questionnaire, we judged to be possible to obtain important data on the disease and its interference in patients’ lives. The goal was to make the treatment easier for both physicians and patients, therefore, increasing the patients’ adherence to the treatment.12,13
Method
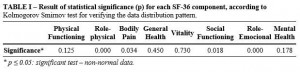
This is a prospective study in which 29 patients were evaluated, 24 females, with a mean age of 14.53 years old. All of them have undergone surgical treatment performed by the Spinal Cord Surgery Group at Hospital Santa Casa de Misericórdia de Vitória (HSCMV). This research project was authorized by the Committee of Ethics for Research in Human Beings of Escola Superior de Ciências da Santa Casa de Misericórdia de Vitória (EMESCAM), under the number 018/2012. The criteria for inclusion were all the AIS patients admitted at HSCMV who presented curves larger than 50 degrees and replied to the quality of life assessment questionnaire SF-36 at pre- and postoperative periods. The criteria for exclusion were some other cause for scoliosis, curves with indication for conservative treatment or patients who did not reply to the assessment questionnaires at the preoperative period. Patients replied to the SF-36 questionnaire preoperatively and 24 months after the surgical treatment. The SF-36 questionnaire may be distributed via computer, telephone or by a trained interviewer and contains 36 items that assess mental and physical health aspects, through 8 components: physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional and mental health. For statistical analysis, we initially applied the Kolmogorov-Smirnov Test, used to assess whether data followed normal distribution, as shown in Table I Source: author. Note: translated. The variables physical functioning, general health, vitality and mental health were normally distributed and correlated, and the Student-t Test was used for paired data. For the non-normal variables, we used the Wilcoxon Test, which is a non-parametric technique similar to the Student-t Test for paired data.14 Values of p ≤ 0.05 were considered statistically irrelevant. The statistical data analysis was performed by using Microsoft Office/Excel 2010 and SPSS (Statistical Package for Social Sciences) version 8.0.
Results
The results showed an improvement in all eight components assessed by the SF-36 questionnaire, comparing the pre- with postoperative periods of patients who have undergone surgery for correcting vertebral scoliosis. When we correlate data obtained from statistical analysis, we found that among the components assessed, physical functioning, role-physical, bodily pain and general health showed statistically relevant improvement at the studied periods, as seen in Table II. Source: author. Note: translated. Among the 8 components studied, physical functioning, role-physical and bodily pain showed higher significance levels during the comparison, reflecting an improvement in the performance of daily activities, including vigorous ones, with decrease or complete relief from pain or pain-related limitations. Despite not having statistical relevance for the social functioning component (p=0.055), the significance level was quite close to 0.05. Regarding the pain component, we observed that 21 patients – 72.74% of the sample – showed some improvement postoperatively, while in the vitality component, only 11 patients noticed improvement after surgery (37.93%).
Discussion
In this paper, we used the SF-36 questionnaire for assessing quality of life in AIS patients due to its easy distribution. This questionnaire can be used for more than 130 diseases, including spinal cord conditions, which may considerably affect the quality of life related to health.15-18 When we analyze the overall result of surgical treatment for AIS via SF-36 questionnaire, it is observed a significant improvement in quality of life even 2 years after the surgical correction. We have decided that this period of time was sufficient for evaluating how the surgical treatment can affect quality of life in these patients. Pellegrino and Avanzi19, in a similar study recently conducted, observed an aggravation in pain and physical functioning in patients at the early postoperative period (up to three months after the surgery), reporting significant improvement when the same patients were reassessed 12 months after the treatment. A very important outcome of this study was the statistically significant improvement in physical functioning, bodily pain and role-physical, similarly to what Cabral et al. have found.17 The Literature reports the incidence of pain in scoliosis is equivalent to the incidence of pain in general population. In this study, we observed a betterment of spinal cord pain in 72.42% of the studied sample, which leads us to conclude that it is necessary to consider its prevalence in these patients. The improvement in the role-physical component assures that scoliosis is a physical problem and has little influence in vitality and mental health. It corroborates with the outcomes we have reached in this study: in spite of showing some improvement, those two components have no statistical relevance. The topic “quality of life” has become particularly important in the analysis of postoperative outcomes for AIS that less aggressive surgeries have been advocated for its treatment, such as selective arthrodesis, in which the goal is to perform the less amount possible of arthrodesis, once stiffness in the spinal cord segment is a constant cause of concern regarding these patients’ quality of life. Despite all the discussion on the topic, we still have not found any study in literature that directly highlights improvement in quality of life with fewer arthrodesis. What we have found indeed is that surgical treatment, when indicated, leads to an improvement in the quality of life of patients regardless the number of levels which have undergone arthrodesis.20
Conclusion
Surgical treatment for AIS has improved all the functional aspects assessed by the SF-36 questionnaire, which actually shows an improvement in the quality of life for these patients.
References
- Weinstein SL. Adolescent Idiopathic Scoliosis: Natural History. In: Weinstein SL. Pediatric Spine, The Principles and Practice. 2nd ed. Iowa: Lippincott Williams & Wilkins; 2001. p.356-67.
- Bunnell WP. The natural history of idiopathic scoliosis. Clin Orthop Relat Res. 1988;229:20-5.
- Beals RK. Nosologic and genetic aspect of scoliosis. Clin Orthop Relat Res. 1973; 93:23-32.
- Cowell HR, Hall JN, MacEwen GD. Genetic aspects of idiopathic scoliosis. Clin Orthop Relat Res. 1972;86:121-31.
- Kouwenhoven JW, Castelein RM. The pathogenesis of adolescent idiopathic scoliosis: review of the literature. Spine (Phila Pa 1976). 2008;33(26):2898-908.
- Ahn UM, Ahn NU, Nallamshetty L, Buchowski JM, Rose PS, Miller NH, et al. The etiology of adolescent idiopathic scoliosis. Am J Orthop (Belle Mead NJ). 2002;31(7):387-95.
- Fowles JV, Drummond DS, L’Ecuyer S, Roy L, Kassab MT. Untreated scoliosis in the adult. Clin Orthop Relat Res. 1978;134:212-7.
- Pehrsson K, Larsson S, Oden A, Nachemson A. Long-term follow-up of patients with untreated scoliosis. A study of mortality, causes of death, and symptoms. Spine (Phila Pa 1976). 1992;17(9):1091-6.
- Weinstein SL, Ponseti IV. Curve progression in idiopathic scoliosis. J Bone Joint Surg Am. 1983;65(4):447-55.
- Danielsson AJ, Wiklund I, Pehrsson K, Nachemson AL. Health-related quality of life in patients with adolescent idiopathic scoliosis: a matched follow-up at least 20 years after treatment with brace or surgery. Eur Spine J. 2001;10(4):278-88.
- Goldberg MS, Mayo NE, Poitras B, Scott S, Hanley J. The Ste-Justine Adolescent Idiopathic Scoliosis Cohort Study. Part II: Perception of health, self and body image, and participation in physical activities. Spine (Phila Pa 1976). 1994;19(14):1562-72.
- Seidl EM, Zannon CM. Quality of life and health: conceptual and methodological issues. Cad Saude Publica. 2004;20(2):580-8.
- Patel AA, Donegan D, Albert T. The 36-item short form. J Am Acad Orthop Surg. 2007;15(2):126-34.
- Siegel S, Castellan Jr. NJ. Estatística Não-Paramétrica Para Ciências do Comportamento. 2ª ed. Porto Alegre: Artmed; 2006.
- Ware JE Jr. SF-36 health survey update. Spine (Phila Pa 1976). 2000;25(24):3130-9.
- Falavigna A, Teles AR, Braga GL de, Barazzetti, DO, Lazzaretti L, Tregnago AC. Instrumentos de avaliação clínica e funcional em cirurgia da coluna vertebral. Coluna/Columna. 2011;10(1):62-67.
- Cabral LTB, Filho ESV, Ueno FH, Yonezaki AM, Rodrigues LMR. Avaliação da qualidade de vida em pacientes com escoliose idiopática do adolescente após tratamento cirúrgico pelo questionário SF-36. Coluna/Columna. 2009;8(3):315-22.
- Patrick DL, Deyo RA, Atlas SJ, Singer DE, Chapin A, Keller RB. Assessing health-related quality of life in patients with sciatica. Spine (Phila Pa 1976). 1995;20(17):1899-908.
- Pellegrino LA, Avanzi O. Prospective Evaluation of Quality of Life in Adolescent Idiopathic Scoliosis before and after Surgery. J Spinal Disord Tech. 2012 Oct 22.
- Negrini S, Grivas TB, Kotwicki T, Maruyama T, Rigo M, Weiss HR, et al. Why do we treat adolescent idiopathic scoliosis? What we want to obtain and to avoid for our patients. SOSORT 2005 Consensus paper. Scoliosis. 2006;1:4.
Acknowledgements
We thank the State of Espírito Santo Research Foundation (FAPES) for the financial support to the fellow scholarship holder of EMESCAM’s Undergraduate Research Internship Institutional Program (originally PIBIC). How to cite this article: Maia T C, Junior C J, Cardoso I M, Brazolino M A N, Junior J L B, Rodrigues J B S R. Evaluation of quality of life in patients who have undergone surgical treatment for idiopathic scoliosis, Salus J Health Sci., [online journal], 2016;2(1). Available at: http://www.salusjournal.org
Attachments
Authors
Thiago Cardoso Maia1*, Charbel Jacob Junior2, Igor Machado Cardoso3, Marcus Alexandre Novo Brazolino4, José Lucas Batista Junior5, João Bernardo Sancio Rocha Rodrigues6 1* Specialist – Resident Doctor at Hospital Municipal Cármino Caricchio, São Paulo, SP. 2 Master’s Degree in Public Policies and Local Development, Escola Superior de Ciências da Santa Casa de Misericórdia de Vitória – EMESCAM, Vitória-ES, Brasil. 3 Specialist in Spinal Cord Surgery, Universidade Estadual de Campinas, São Paulo, SP. 4 Specialist – Resident Doctor at Instituto de Assistência Médica ao Servidor Público Estadual, São Paulo, SP. 5 Specialist – Resident Doctor at Santa Casa de Misericórdia de Juiz de Fora – MG. 6 Specialist – Resident Doctor at Instituto de Previdência dos Servidores do Estado de Minas Gerais. MG. Article received on June 21 2015 Article accepted on August 27 2015
