


CARDIAC AND BLOOD PRESSURE EFFECTS OF LEAD EXPOSURE
Abstract
Objective: To construct a review on cardiac effects and blood pressure of lead exposure. Method: This is a structured narrative review in three distinct phases: 1) elaboration of the guiding question: “What are the cardiac and blood pressure effects of lead exposure?”; 2) Sampling in the literature and selection of studies; 3) Critical analysis of selected studies. Results: several aspects related to cardiac effects and blood pressure of lead exposure were obtained, among them: arterial hypertension, autonomic dysregulation, dysregulation of myocardial contractility, increase in ventricular overload, increase in afterload and of the pulse pressure. Furthermore, the evidence is suggestive of an association between exposure to lead and mortality from cardiovascular causes, particularly related to ischemic heart disease. Conclusion: researchers on the subject warn that exposure to lead is reasoned as a cardiovascular risk factor.transplantation will be used.
Introduction
Lead is a toxic metal and an environmental pollutant used in the manufacture of batteries, paints, ceramics, crystals, cables, ammunition and high-tech products, such as nuclear reactor protectors and thin plates of electronic components.1
Although several countries adopt measures to reduce the emission of lead, environmental contamination by this metal still remains a public health problem.2 The World Health Organization (WHO) estimates that 140,000 people die every year, due to contamination by this metal, in addition to causing 600,000 cases of intellectual loss in children.2
Several studies have documented the adverse effects of lead exposure in the adult population and in children.3-5 Young children are particularly vulnerable to the toxic and, in some cases, permanent effects of lead, especially by affecting the nervous system.6 Studies indicate an association between blood lead concentration and development of hypertension, gastrointestinal disorders, as well as renal and cardiovascular dysfunctions.1,6
Considering the toxic potential of lead, this article seeks to compile information from the scientific literature and to support the construction of a reference on cardiac toxicity and the effects on blood pressure on exposure to this metal.
Method
This is a narrative review related to cardiac toxicity and the effects on blood pressure of lead exposure. We chose this type of literature review that allows the incorporation of evidence for convenience, for an expertise in the theme, in order to build a body of knowledge about a certain topic of scientific relevance.
The review process was systematized in three distinct phases, the first of which was the elaboration of the guiding question: “What are the cardiac effects and blood pressure of lead exposure?”. The second phase corresponded to sampling in the literature, which sought to include the largest possible variety of identified products and ensure the variety and breadth of results.
In this sense, electronic selection was performed in the databases of LILACS (Latin American and Caribbean Literature) and MEDLINE (National Library of Medicine, USA). The electronic search was performed through the following combinations of Descriptors in Health Sciences (DeCS): “lead; toxicity; heart; Arterial pressure” and was based on the adoption of the following inclusion criteria: the indexing of studies in the respective databases in Portuguese, English and Spanish. Exclusion criteria were defined as: productions without availability of text in full or with a central theme of the study, unrelated to the topic of cardiac toxicity and effects on blood pressure in lead exposure.
The third phase of this review consisted of a critical analysis of the selected studies. The decision to include or reject the studies was based on the reading of the titles of the selected studies, followed by the critical analysis of the abstracts, and the studies with a central theme unrelated to the theme proposed for the review were rejected. In a second analysis, we verified the content in its entirety, which was guided by the thematic analysis technique to identify the central ideas presented.
Results / Discussion
In order to inform and contribute to analyzes and debates about the effects of exposure to lead, heart and blood pressure, the contents that make up the review were stratified in the following categories.
– Exposure to lead and hypertension
Population studies of the cardiovascular effects of lead are focused on the development of arterial hypertension while studies with experimental animals seek to elucidate the mechanisms involved in cardiovascular changes.4,7-12
Several clinical and epidemiological studies point to an association between exposure to lead and high blood pressure. However, only recently has it been shown that blood lead concentration below the limits considered safe for human health,13,14 or exposure to a single dose of metal,15 are able to raise the systolic blood pressure of experimental animals.
It is believed that the pathogenesis of lead toxicity in the development of hypertension is multifactorial, as: alter calcium homeostasis,9,14,16 promote sympathetic hyperactivity,14,17 induce increased renin-angiotensin system activity15,18 to depress the antioxidant reserves of the organism and/or increase the production of reactive oxygen species (ROS), resulting in oxidative stress,7,19,20 alter the vascular response to vasoactive agents,13,21 promote endothelial damage, reduce bioavailability of nitric oxide and increase endothelin levels11,22 besides inducing renal damage.23
– Exposure to lead and autonomic deregulation
Autonomic imbalance, characterized by hyperactivity of the sympathetic system and hypoactivity of the parasympathetic system, is associated with several pathological conditions that may favor the onset or aggravate cardiovascular diseases.24-28 Some clinical and animal studies have focused on the Sympathetic system as a possible mediator of hypertension and cardiovascular diseases induced by lead exposure.
GUMP et al,25 studied the cardiovascular response to acute stress in children exposed to low prenatal concentrations of lead and to low concentrations of this metal during childhood. These authors showed that the highest blood concentrations of lead are associated with higher systolic pressures and increased peripheral vascular resistance and, consequently, increased cardiac overload. Moreover, the blood concentration of lead was associated with a reduction in systolic volume and cardiac output, which were associated with a reduction in cardiac autonomic dysregulation.26
In adults, PARK and co-workers have shown that chronically exposed people may be more susceptible to cardiac autonomic dysfunction.27,28 In experimental animals, sympathetic hyperactivity and its inotropic and chronotropic consequences in lead exposure are well documented.9,14,17 Elevation of plasma norepinephrine and reduction of β-adrenergic receptor density are the two best mechanisms reported in interference in the autonomic regulation of lead exposure.
– Exposure to lead and elevation of pulse pressure
Chronic exposure to lead is associated with increased pulse pressure, a marker of arterial stiffness, and an indicator of cardiovascular disease. ZANGH et al.29 studied 619 participants of the Normative Aging Study in the United States of America and demonstrated that H63D gene polymorphism of hemochromatosis (which may alter lead deposition and hence its cardiotoxic effect) increases susceptibility to deleterious effects of Lead in the pulse pressure. The increase of the pulse pressure is attributed to progressive arterial stiffness and consequent alteration in vascular structure and function with degradation of elastin, increase of collagen, calcification and atherosclerosis. These effects are made possible by pro-oxidative or pro-inflammatory mechanisms that occur in lead exposure, since lead induces oxidative stress and this can promote direct damage in different organs and systems, including the heart itself.30 The mechanisms by which Lead induces oxidative stress include lipid peroxidation in membranes, damage to the DNA and antioxidant system of the organism resulting in greater generation and/or availability of free radicals.7,21,31
– Exposure to lead and disturbances in myocardial contractility
Vassallo et al.32 studied isolated right ventricle strips submitted to acute lead exposure and recorded reduction of isometric strength and indicated lead as a risk factor capable of altering cardiac function. Later, Fioresi et al.9 investigated the acute effects of lead in the isometric contraction of isolated papillary muscles of the left ventricle of rats and demonstrated that the increase in ventricular pressure induced by acute exposure to lead has, besides vascular involvement, direct changes in myocardial contractility.
Fioresi et al.14 showed that a blood concentration of lead, below the limits considered safe, results in an increase in blood pressure, HR and left ventricular inotropism, in addition to promoting changes in the calcium cycle of the cardiomyocyte, which may contribute to the deleterious effects of this metal on the heart.
Figure 1 shows the mechanisms by which lead, in the treatment model used by Fioresi et al,14 alters the calcium cycle in the cardiomyocyte: there is a greater influx of transarcolemal calcium, but this higher influx does not result in positive inotropism, since the sarcoplasmic reticulum calcium pump (SERCA 2) is desensitized and the sodium-calcium exchanger (NCX) promotes the extrusion of these ions from the cell.
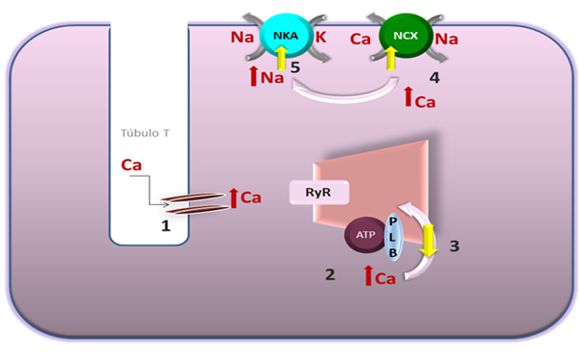
Figure 1: Mechanism proposed by which exposure to lead changes the calcium cycle in the cardiomyocyte. 1: Lead promotes greater influx of transarcolemal calcium; 2: There is an increase in [Ca] i; 3: There is desensitisation of SERCA 2 and less calcium reuptake; 4: Consequently, the increase in [Ca]i activates NCX to remove cytosolic calcium; 5: Increased NCX activity results in an increase in [Na]i, which in turn activates NKA.
– Exposure to lead and cardiovascular mortality
Several studies associate the blood concentration of lead to mortality. Weisskopf et al,33 studied 868 men participating in the Normative Aging Study in the United States of America and found an association between lead bone content and cardiovascular mortality in the chronically exposed population at low blood concentrations of this metal. This association between lead exposure and mortality due to cardiovascular causes is particularly related to ischemic heart disease.34 Although cardiac ischemic disease is multifactorial, exposure to lead may represent a risk factor that contributes to this outcome.34
There are several deleterious cardiovascular effects triggered by exposure to lead which, in combination, may lead to increased cardiovascular mortality.4 Among these effects are: interference in cardiac contractility;9,14,32 increase in vascular tone and peripheral resistance;19 stimulation of the renin-angiotensin system;15,18 reduction in the availability of nitric oxide and increased oxidative stress;13,35 interference in the cardiac autonomic control.36
Conclusion
Lead has toxic effects on the heart and exposure to this metal may be considered a cardiovascular risk factor, since several studies point to a causal relationship between this exposure and the development of hypertension.
There is sufficient evidence that chronic exposure to lead has deleterious cardiac effects by affecting autonomic regulation and promoting ventricular overload, by increasing pressure afterload and pulse pressure. Furthermore, the evidence is suggestive of an association between exposure to lead and mortality from cardiovascular causes, particularly related to ischemic heart disease.
Although there is a need for further research, especially clinical and epidemiological studies, to clarify the effects and mechanisms involved in lead cardiotoxicity, it is essential for the responsible public agencies to reevaluate the safe exposure values and that the investigation of exposure to this metal to be routinely included in the cardiovascular research, mainly in workers occupationally exposed to lead.
References
- Koh DH , Locke SJ, Chen YC, Purdue MP, Friesen MC. Lead exposure in US worksites: A literature review and development of an occupational lead exposure database from the published literature. Am J Ind Med. 2015 Jun, 58(6): 605–16.
- World Health Organization (WHO). (2014) International Lead Poisoning Prevention Week 2014. Disponível em:
- Den HE, Nawrot T, Staessen JA. The relationship between blood pressure and blood lead in NHANES III. J Hum Hypertens. 2002 Aug;16(8):563-8.
- Navas-Acien A, Guallar E, Silbergeld EK, Rothenberg SJ. Lead Exposure and Cardiovascular Disease- A Systematic Review. Environ Health Perspect. 2007 Mar;115(3):472-82.
- Vupputuri S, He J, Muntner P, Bazzano LA, Whelton PK, Batuman V. Blood Lead Level Is Associated With Elevated Blood Pressure in Blacks. Hypertension. 2003 Mar;41(3):463-8.
- World Health Organization (WHO). (2015) Lead Poising and health. Disponível em:
- Farmand F, Ehdaie A, Roberts CK, Sindhu RK. Lead-induced dysregulation of superoxide dismutases, catalase, glutathione peroxidase, and guanylate cyclase. Environ Res. 2005 May;98(1):33-9.
- Sharifi AM, Darabi R, Akbarloo N, Larijani B, Khoshbaten A. Investigation of circulatory and tissue ACE activity during development of lead-induced hypertension. Toxicol Lett. 2004 Nov 2;153(2):233-8.
- Fioresi M, Furieri LB, Simões MR, Ribeiro RF Jr, Meira EF, Fernandes AA, Stefanon I, Vassallo DV. Acute exposure to lead increases myocardial contractility independent of hypertension development. Braz J Med Biol Res. 2013 Feb;46(2):178-85.
- Fiorim J, Ribeiro RF Jr, Azevedo BF, Simões MR, Padilha AS, Stefanon I, et al. Activation of K+ channels and Na+/K+ ATPase prevents aortic endothelial dysfunction in 7-day lead-treated rats. Toxicol Appl Pharmacol. 2012 Jul 1;262(1):22-31.
- Silveira EA, Siman FD, de Oliveira Faria T, Vescovi MV, Furieri LB, Lizardo JH, et al..Low-dose chronic lead exposure increases systolic arterial pressure and vascular reactivity of rat aortas. Free Radic Biol Med. 2014 Feb;67:366-76.
- Simões MR, Aguado A, Fiorim J, Silveira EA, Azevedo BF, Toscano CM, et al. MAPK pathway activation by chronic lead-exposure increases vascular reactivity through oxidative stress/cyclooxygenase-2-dependent pathways. Toxicol Appl Pharmacol. 2015 Mar 1;283(2):127-38.
- Fiorim J, Ribeiro Júnior RF, Silveira EA, Padilha AS, Vescovi MV, de Jesus HC, et al. Low-level lead exposure increases systolic arterial pressure and endothelium-derived vasodilator factors in rat aortas. PLoS One. 2011 Feb 25;6(2):e17117.
- Fioresi M, Simões MR, Furieri LB, Broseghini-Filho GB, Vescovi MV, et al. Chronic lead exposure increases blood pressure and myocardial contractility in rats. PLoS One. 2014 May 19;9(5):e96900.
- Simões MR, Ribeiro Júnior RF, Vescovi MV, de Jesus HC, Padilha AS, Stefanon I, et al. Acute lead exposure increases arterial pressure: role of the renin-angiotensin system. PLoS One. 2011 Apr 11;6(4):e18730.
- Valencia I, Castillo EE, Chamorro G, Bobadilla RA, Castillo C. Lead induces endothelium- and Ca2+- independent contraction in rat aortic rings. Pharmacol Toxicol. 2001 Oct;89(4):177-82.
- Carmignani M, Volpe AR, Boscolo P, Qiao N, Di Gioacchino M, Grilli A, et al. Catecholamine and nitric oxide systems as targets of chronic lead exposure in inducing selective functional impairment. Life Sci. 2000 Dec 15;68(4):401-15.
- Sharifi AM, Darabi R, Akbarloo N, Larijani B, Khoshbaten A. Investigation of circulatory and tissue ACE activity during development of lead-induced hypertension. Toxicol Lett. 2004 Nov 2;153(2):233-8.
- Silveira EA, Lizardo JH, Souza LP, Stefanon I, Vassallo DV. Acute lead-induced vasoconstriction in the vascular beds of isolated perfused rat tails is endothelium-dependent. Braz J Med Biol Res. 2010 May;43(5):492-9.
- Nunes KZ, Nunes DO, Silveira EA, Almenara Cruz Pereira C, Broseghini Filho GB, Vassallo DV, et al. Chronic lead exposure decreases the vascular reactivity of rat aortas: the role of hydrogen peroxide. PLoS One. 2015 Mar 25;10(3):e0120965
- Zhang LF, Peng SQ, Wang S. Influence of lead (Pb2+) on the reactions of in vitro cultured rat aorta to 5-hydroxytryptamine. Toxicol Lett. 2005 Oct 15;159(1):71-82.
- Grizzo LT, Cordellini S. Lead Exposure Affects Nitric Oxide and Cyclooxygenase Pathways in Aorta of Weaned Rats. Toxicol Sci. 2008 May;103(1):207-14.
- Roncal C, Mu W, Reungjui S, Kim KM, Henderson GN, Ouyang X, et al. Lead, at low levels, accelerates arteriolopathy and tubulointerstitial injury in chronic kidney disease. Am J Physiol Renal Physiol. 2007 Oct;293(4):F1391-6.
- Thayer JF, Yamamoto SS, Brosschot JF. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int J Cardiol. 2010 May 28;141(2):122-31.
- Gump BB, Stewart P, Reihman J, Lonky E, Darvill T, Matthews KA, et al. Prenatal and early childhood blood lead levels and cardiovascular functioning in 9 1/2 year old children. Neurotoxicol Teratol. 2005 Jul-Aug;27(4):655-65.
- Gump BB, Mackenzie JA, Bendinskas K, Morgan R, Dumas AK, Palmer CD, et al. Low-level Pb and Cardiovascular Responses to Acute Stress in Children: The Role of Cardiac Autonomic Regulation. Neurotoxicol Teratol. 2011 Mar-Apr;33(2):212-9.
- Park SK, Schwartz J, Weisskopf M, Sparrow D, Vokonas PS, Wright RO, et al. Low-Level Lead Exposure, Metabolic Syndrome, and Heart Rate Variability: The VA Normative Aging Study. Environ Health Perspect. 2006 Nov;114(11):1718-24.
- Park SK, O’Neill MS, Vokonas PS, Sparrow D, Wright RO, Coull B, et al. Air Pollution and Heart Rate Variability: Effect Modification by Chronic Lead Exposure. Epidemiology. 2008 Jan;19(1):111-20.
- Zhang A, Park SK, Wright RO, Weisskopf MG, Mukherjee B, Nie H, et al. HFE H63D Polymorphism as a Modifier of the Effect of Cumulative Lead Exposure on Pulse Pressure: The Normative Aging Study. Environ Health Perspect. 2010 Sep;118(9):1261-6.
- Ahamed M, Siddiqui MK.Low lead exposure and oxidative stress: Current opinions. Clin Chim Acta. 2007 Aug;383(1-2):57-64.
- Courtois E, Marques M, Barrientos A, Casado S, López-Farré A. Lead-Induced Downregulation of Soluble Guanylate Cyclase in Isolated Rat Aortic Segments Mediated by Reactive Oxygen Species and Cyclooxygenase-2. J Am Soc Nephrol. 2003 Jun;14(6):1464-70.
- Vassallo DV, Lebarch EC, Moreira CM, Wiggers GA, Stefanon I. Lead reduces tension development and the myosin ATPase activity of the rat right ventricular myocardium. Braz J Med Biol Res. 2008 Sep;41(9):789-95.
- Weisskopf MG, Jain N, Nie H, Sparrow D, Vokonas P, Schwartz J, et al. A Prospective Study of Bone Lead Concentration and Death From All Causes, Cardiovascular Diseases, and Cancer in the Department of Veterans Affairs Normative Aging Study. Circulation. 2009 Sep 22;120(12):1056-64.
- Jain NB, Potula V, Schwartz J, Vokonas PS, Sparrow D, Wright RO, et al. Lead levels and ischemic heart disease in a prospective study of middle-aged and elderly men: the VA Normative Aging Study. Environ Health Perspect. 2007 Jun;115(6):871-5.
- Vaziri ND, khan M. Interplay of reactive oxygen species and nitric oxide in the pathogenesis of experimental lead-induced hypertension. Clin Exp Pharmacol Physiol. 2007 Sep;34(9):920-5.
- Simões MR, Preti SC, Azevedo BF, Fiorim J, Freire DD Jr, Covre EP, et al. Low-level Chronic Lead Exposure Impairs Neural Control of Blood Pressure and Heart Rate in Rats. Cardiovasc Toxicol. 2016 Jun 7.
Authors
Mirian Fioresi1; Maylla Ronacher Simões2; Karolini Zuqui Nunes3; Jonaína Fiorim4; Edna Aparecida Silveira5
1 Department of Nursing, Federal University of Espírito Santo, Vitoria, ES, Brazil
2,3 Department of Physiological Sciences, Federal University of Espírito Santo, Vitoria, ES, Brazil.
4,5 Physiotherapists at the Hospital Universitário Cassiano Antônio Moraes, HUCAM.
