


THYROID FUNCTION DISORDERS INDUCED BY AMIODARONE
Abstract
Amiodarone is an antiarrhythmic rich in iodine and a medication prescribed in clinical practice for the treatment of cardiac arrhythmias. Its use is related to dysfunction in various organs such as the thyroid gland. It is known that most patients remain euthyroid, but some dysfunctions, for instance hypothyroidism and thyrotoxicosis type I and II, may occur in 15 to 20%, being hypothyroidism more frequent. The treatment for this issue is levothyroxine. The treatment depends on the type of thyrotoxicosis diagnosed in the patient. It is therefore necessary to screen for the diagnosis and treatment of thyroid dysfunction early and effectively, since the permanence of these dysfunctions may lead to a worsening of the heart function of the patient.
Introduction
Amiodarone was introduced in clinical practice in the 60’s, initially as an antianginal agent, and later studies of its electrophysiological effects established its use as an antiarrhythmic agente,1 being widely used specially in refractory arrhythmias to conventional treatment.2
This drug has a chemical structure similar to thyroid hormones: triiodothyronine (T3), thyroxine (T4), Reverse T3 and its active metabolite, desethylamiodarone (DEA). Each amiodarone molecule has two iodine atoms, which corresponds to 37% of its molecular weight. 3,4
Regarding thyroid gland dysfunction, hypothyroidism and type I and II thyrotoxicosis, it is estimated that 15% to 20% of patients under the medication develop these effects. This percentage raises to 50% over four years of treatment.1 These secondary effects may linger for months after discontinuation of the drug, a fact that is due to its long half-life and storage capacity in adipose tissue.
Thus, when starting the use of the drug, it is of great importance to perform a complete medical history and watch over laboratorial parameters. This makes it possible to assess and identify patients predisposing the development of thyroid dysfunction.
It is known that in average, 10% of the molecule is deiodinated on a daily basis and the drug maintenance dose ranges between 200mg to 600mg per day. Thus, the amount of iodine available in the body ranges between 7mg to 21mg daily. This amount is higher than the daily intake of iodine recommended by WHO, which is 0,15mg to 0,3mg per day.5
Amiodarone action mechanisms in thyroid physiology
Amiodarone interference in the thyroid hypothalamic-pituitary axis is due to intrinsic effects of the drug and its iodine content.
Iodine, substrate for the synthesis of thyroid hormones, is transported to inside thyroid follicular cell where it will be organified. This process is self-regulated to avoid iodine overcharge. In a situation of iodine excess, the synthesis of thyroid hormones is inhibited and this process is known as Wloff-Chaikoff effect, which is transitory and followed by an escape mechanism.
In cases of thyroid autoimmune disease, there are, many times, defects in this self-regulation with failure of the escape mechanism.4,6,7 The explanation for the development of this condition would be an inhibition of the synthesis of thyroid hormones resulting from iodine overload due to metabolization of amiodarone, leading to hypothyroidism. Iodine excess can also lead to a potentiation of thyroid autoimmunity and increased synthesis of thyroid hormones (Jod-Basedow effect) in patients with Graves’ disease or nodular goiter, leading to hyperthyroidsm.4
Regarding the intrinsic action of amiodarone, there is deiodinase inhibition at central and peripheral level, block of peripheral uptake of thyroid hormones, direct cytotoxicity to thyroid and decreased binding of T3 to its receptor.
At peripheral tissues, mainly liver, thyroid and kidney, amiodarone inhibits the action of type I deiodinase enzyme, responsible by peripheral conversion of T4 into T3, as well as reverse T3 (rT3) into diiodothyronine (T2). This is probably due to a mechanism of competitive antagonism due to the similarity with the T4 structure.2
There is also an inhibition of activity of enzyme deiodinase type II (DIO2) which operates at pituitary level converting T4 into T3. After discontinuation of the drug, this inhibitory effect can persist for several months. In addition to enzyme inhibition, amiodarone also blocks the entry of thyroid hormones in peripheral tissues.5 Both described mechanisms lead to increased serum concentrations of T4 and rT3, besides the decrease of T3. However, most patients remain clinically euthyroid.2
Regarding the TSH values, the changes observed with use of amiodarone are time and dose dependent. The increase in plasma TSH initially occurs in response both to the fall in the concentration of T3 in central level (by inhibition of the deiodinase type 2) and to the connection of DEA to intracellular receptors T3, antagonizing it.8
Thyroid cytotoxicity may occur by direct action of amiodarone, resulting in destructive thyroiditis, as well as by the excess of iodine present in the drug, inducing phenomena of apoptosis and oxidative stress.9
Regarding to thyroid autoimmunity, studies show that it is unlikely that treatment with amiodarone triggers the appearance of autoantibodies. However, it may precipitate or worsen pre-existing autoimmunity in susceptible individuals, since most patients who develop amiodarone-induced hypothyroidism has positive values of antithyroid autoantibodies before treatment.5,10
The appearance of thyroid dysfunction induced by amiodarone may be related to predisposing factors such as dietary iodine ingestion, presence of personal and/or family history of thyroid disease and presence of antithyroid antibodies prior to use of the drug.
The thyrotoxicosis is more frequent in regions with insufficient iodine intake, whereas hypothyroidism is found in areas with sufficient iodine supply. The overall incidence of thyroid dysfunction in patients using amiodarone ranges from 14% to 18%, and the incidence for hyperthyroidism ranging from 5% to 10% and hypothyroidism 10% to 20%.4 In the United States, the cases of hypothyroidism are more prevalent, compared to thyrotoxicosis, whereas in Europe this correlation is the inverse.2
Amiodarone-induced hypothyroidism
Amiodarone-induced hypothyroidism occurs earlier if compared to hyperthyroidism and its development is independent of the daily doses of the drug. It is observed an association with advanced age, female gender and autoimmune thyroid disease.8 Therefore, the dosage of antithyroid antibodies, especially antiperoxidase antibodies (anti-TPO) should be given, as are markers of autoimmune thyroid disease.
Previous occurrence of Hashimoto’s thyroiditis is an established risk factor for the occurrence of hypothyroidism,2 which occurs generally between 6 to 12 months of amiodarone use.
Additionally, the extra intake of iodine, added to the previous presence of autoantibodies, can lead to the destructive thyroiditis phenomena. The clinical manifestations of amiodarone-induced hypothyroidism are weight gain, weakness, hair loss, dry skin, cold intolerance and lethargy, this one being the most common. These signs and symptoms are, in majority, difficult to diagnose, once it can be attributed to the heart disease in these patients. Goiter and myxedema are uncommon.9
The hypothyroidism diagnosis is usually simple. Laboratory characteristics include high levels of TSH, usually above 20mU/L, associated to reduced free T4 (FT4) values.8 However, it can be observed a subclinical form of the disease, with moderately elevated TSH (levels between 4,3mU/L and 20mU/L) and normal FT4.9
In patients with subclinical hypothyroidism, the levothyroxine (L-T4) treatment should be taken if there are antithyroid antibodies present. Symptomatic patients with no antibodies should be re-evaluated in three months. Evaluation should be made in frequent intervals (six weeks and later in every three months) in case of absence of antibodies and symptoms.11
The TSH serum level constitutes the first-line test for hypothyroidism diagnosis. However, it is necessary to consider the TSH increase that occurs in the first three months of amiodarone therapy. The free T3 (FT3) levels have no use for diagnosis.9
Hypothyroidism treatment by amiodarone is based on levothyroxine use. Initially in low doses (25mcg to 50mcg) with posterior gradual increase.
Interruption of drug intake brings little benefit. However, on patients who need to keep the drug use, there is need of a higher levothyroxine dose if compared to other hypothyroidism conditions. Higher doses should be considered in some situations such as obesity, children and young adult, severe hypothyroidism, jejunoileal bypass post-surgery and cirrhosis.4 On the other hand, in patients in which can discontinue the drug use, it is known that hypothyroidism is transitory and may revert spontaneously, being indicated mainly in symptomatic patients.4 In these cases it should be re-evaluated the need to continue therapy or to adjust doses between six to twelve months after commencement of reposition.9
TSH is the most important parameter to monitor this therapy,2 being recommended the dosage every four to six weeks.4 It is appropriate to maintain the TSH levels at the upper limit of normality, especially in patients with severe cardiopathy.3 You can reach the euthyroid state in two to four months after discontinuation of amiodarone.5 After normalization of thyroid hormones, laboratory monitoring could be done in every six to twelve months.4
Amiodarone-induced thyrotoxicosis
Thyrotoxicosis, potentially grave and unpredictable situation, is more common in areas deficient in iodine, male gender (3:1), young people and patients with previous thyroid pathology, although it may affect normal thyroid tissue.5 Its appearance is not dependent on amiodarone doses, just as it is observed in hypothyroidism.
Two subtypes of amiodarone-induced thyrotoxicosis are described, which differ regarding etiology, prognosis and treatment.
The type I thyrotoxicosis occurs in patients with underlying thyroid disease, such as self-nodular goiter and Graves’ disease, and is a consequence of Jod Basedow phenomena (iodine induced hyperthyroidism), typical of geographic regions with deficiency on dietary iodine.12
The Type II thyrotoxicosis occurs in normal thyroid tissue, caused by a direct thyroid destruction by amiodarone or its metabolites (subacute destructive thyroiditis). This fact results in release of preformed thyroid hormones into the circulation. Because of this destructive process after the state of thyrotoxicosis, a transient hypothyroidism can be observed.9
It should be remembered that both forms may be associated, being difficult to distinguish them. The clinical presentation is similar in both types of hyperthyroidism and can manifest with weight loss, excessive sweating, hyperkinesia, muscle weakness, heat intolerance, diarrhea and hair loss. The ophthalmopathy is usually absent unless hyperthyroidism develop in a patient with previous Graves’ disease.9 The differential diagnosis, therefore, involves clinical, laboratory and imaging parameters.
The evaluation should include a detailed medical history and physical examination to determine if the patient has a pre-existing thyroid disease such as nodular goiter, or Graves’ disease, which suggests hyperthyroidism type I.4
The detection of antibodies antiTPO and Thyroid Stimulating Hormone Receptor Antibodies (TRAb) which are generally absent, helps to differentiate patients with a previous thyroid condition, suggesting hyperthyroidism type I.5
Conventional ultrasound can help detect structural changes, such as a nodular goiter or an enlarged gland, but does not allow to distinguish the types of hyperthyroidism.2 However, the colored Doppler flow ultrasound is an inexpensive method of quick and easy implementation, non-invasive and effective in distinguishing the two types of hyperthyroidism.2 The hypervascularity evidence is suggestive of type I hyperthyroidism, while its absence was associated with type II hyperthyroidism.3
The utilization of thyroid scintigraphy with radioactive iodine (RAIU) can help differentiate the two types of hyperthyroidism. The uptake is typically normal or high in type I; In the type II, it is observed a reduced uptake, since there is little absorption of iodine due to destruction and damage in thyroid tissue.
The dosage of interleukin 6 (IL-6) is a good marker of destruction of the thyroid follicular epithelium, although it is not specific. The levels are normal or slightly elevated in type I and significantly elevated in type II.3
It is worthy to note that none of the proposed diagnostic methods is able to distinguish the two kinds of hyperthyroidism by itself, requiring the combination of different techniques.9 The main clinical and laboratory characteristics to differentiate types of hyperthyroidism are summarized in Table 1.
Table 1 – Diferential diagnosis of the amiodarone-induced thyrotoxicosis forms (3)
| Characteristics | Type I | Type II |
| Previous thyroid disorder | Yes | No |
| Nodular or diffuse goiter | Frequently present | Usually absent |
| Antithyroid antibodies | Frequently present | Absent |
| Radioactive iodine uptake | Low, normal or high | Low / suppressed |
| Serum IL-6 | High, discreetly | Very high |
| Doppler ultrasound | Hyperflow signs | Low flow signs |
| Thyroid ultrasound | Goiter (diffuse or nodular) | Normal |
Note: adapted by the authors.
The treatment of amiodarone-induced hyperthyroidism is a challenge, being non unanimous among health professionals. The most controversial treatment option consists in the suspension, or not, of amiodarone. In cases where the interruption is possible, the replacement by another drug is an acceptable condition. However, the suspension is not accompanied by immediate effect due to the long half-life of the drug.8
In general, in less harmful forms of hyperthyroidism, 20% of cases have spontaneous remission.5 However, in most cases, treatment is needed once the thyroid hormones are deleterious on the heart disease of the patients.
In type I hyperthyroidism, the main objective is to inhibit the synthesis of thyroid hormones. Thionamides are the drugs of choice because they block the hormonal synthesis,4 besides to peripherally inhibit the deiodinase enzyme, effect observed only in propylthiouracil (PTU).8 It is commonly used in higher doses (methimazole 40-60mg/day or propylthiouracil 600mg to 800mg/day),5 because excess of iodine in the thyroid gland, from the intake of amiodarone, confers resistance to the action of thyonamide. The dosage is gradually decreased to lower maintenance values.12
Methimazole is the drug used as first-line, due to the possibility of ingestion once per day (half-life longer than propylthiouracil), faster normalization of hormone levels and lower incidence of side effects (cutaneous and gastrointestinal manifestations, arthralgia, agranulocytosis, hepatotoxicity and vasculitis). Due the chance of occurring bone marrow suppression, patients should be counseled about the warning signs, such as fever, sore throat and ulcers in oral cavity. The side effects associated with methimazole are dose dependent, as propylthiouracil is not dose dependent.4
It can be used together with this therapy the potassium perchlorate (1g/day), which is capable of inhibiting the uptake of iodine, improving the effectiveness of thionamides. Doses higher than 1g/day are associated with the occurrence of agranulocytosis and aplastic anemia.5 The toxicity limits their use and patients using thyonamide and potassium perchlorate should do a blood test every 15 days. The interruption of potassium perchlorate administration should occur when the euthyroid state is reached, typically after six weeks.4
Lithium carbonate (900mg-1350mg / day, 4 to 6 weeks), by owning action in synthesis reduction and hormone secretion, can be an alternative in more severe cases or refractory to initial treatment,5 which can be associated with thyonamide.
In hyperthyroidism type II treatment, thyonamide and potassium perchlorate are not indicated, because it is about a destructive thyroiditis. Therefore, it is preferable the use of corticosteroids due to their anti-inflammatory and membrane stabilizer effects, and inhibition of peripheral conversion of T4 into T3.2 Different types of corticosteroids may be used, such as prednisone (15mg-80mg daily), and dexamethasone (3mg, 6mg daily)5 for two to three months.4,13
The treatment with radioactive iodine (13II) is usually not possible due to low or suppressed uptake of this isotope; however, it can be used in the definitive treatment in the few patients with evidence of a high uptake (high RAIU).14
When hyperthyroidism is resistant to treatment and it is urgent to restore euthyroid state, there are other alternatives: plasmapheresis and thyroidectomy.4 The total thyroidectomy is an option indicated in the definitive treatment of both forms of thyrotoxicosis8 in the following situations: patients resistant to initial therapy; adverse reactions to treatment; Patients with severe symptoms; impossibility of amiodarone suspension and in cases of deterioration of cardiac function.9 It must be done a control of thyrotoxicosis before surgery through the use of iopanoic acid. This fact is associated with reduction of surgical risk of cardiac patients,16 but this drug is no longer available for us.5
It is important to emphasize that hyperthyroidism types I and II may be associated. A form known as thyrotoxicosis type III or mixed. The treatment proposed in this case is the combination of methimazole, potassium perchlorate, and corticosteroids. This is the most beneficial type of treatment.5
The question of whether or not to discontinue amiodarone, in the case of hyperthyroidism, must be based on cardiac criteria. This drug is extremely effective as an antiarrhythmic and in some patients the suspension may lead to some risks. Other than that, amiodarone blocks the beta-adrenergic receptor and antagonizes the thyroid hormone receptors, performing a heart protective effect, which when removed, may worsen heart condition. However, it is recommended to stop amiodarone use whenever possible, whether in the case type I or type II.2,3,16-18
Thyroid function monitoring while using amiodarone
Clinical and laboratory evaluation of thyroid function should be performed before, during and after amiodarone use. It is necessary to care about this mainly because of the frequent thyroid alterations observed in this group of patients, besides the possibility of worsening previous cardiac function.
The first evaluation is composed by a detailed medical history, physical examination which includes thyroid gland palpation. This trial seeks to keep track of patients with higher risk to develop thyroid pathologies. The presence of diffuse nodular goiter points to a higher predisposition to hyperthyroidism, as well as the presence of antiTPO antibodies is associated to the occurrence of hypothyroidism.10
Another initial care is the dose of TSH, FT4 and antiTPO antibodies. It is worthy to point that thyroid function should be evaluated every six months or in presence of clinical alterations that develop along treatment.8 Besides, screening should continue even after drug withdrawal, due to its long half-life.9 Patients with higher predisposition to gland alterations should have an individualized and thorough evaluation interval.9
TSH dose is considered the best test to monitor thyroid function, although euthyroid patients on amiodarone use may have reduced TSH levels.10 The management and monitoring of thyroid function are summarized in Picture 1.
Picture 1 – Thyroid function monitoring regarding amiodarone use (9)
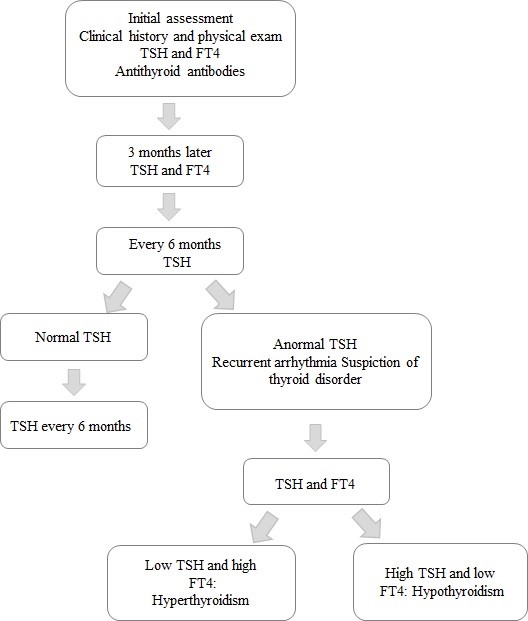
Source: LOPES, Z. M. T. C. Patologia da tireoide associada ao consumo de amiodarona. 2013. 40 f. Dissertação (Mestrado em Medicina) – Faculdade de Medicina, Universidade da Beira do Interior, Covilhã, 2013.
The detailed flowchart above shows the steps to be followed in the clinical monitoring of thyroid function of a patient using amiodarone, and how to diagnose and changes in thyroid function when suspecting a thyroid disorder.
Conclusion
Amiodarone induces changes in thyroid function tests which are, mostly, explained by the excess of iodide and inhibition of deiodinase activity. Clinically relevant thyroid dysfunction is not uncommon during therapy with amiodarone, but requires careful diagnosis and treatment.
The frequency with which amiodarone causes thyroid dysfunction, as well as other complications, should be observed to emphasize the need for monitoring. It should include the TSH dose both before the introduction of amiodarone as well as long-term serial actions.
References
- Toni M, Anda E, Pineda J, Martinez de Esteban JP, Ollero MD. The effects of amiodarone on the thyroid. An Sist Sanit Navar. 2009; 32(3): 363-70.
- Campos MV. Efeitos da amiodarona na tireóide: aspectos actuais. Acta Méd Port. 2004; 17: 241-246.
- Pavan R, Jesus AMX, Maciel LMZ. A amiodarona e a tireóide. Arq Bras Endocrinol Metab, 2004; 48(1): 176-82.
- Marques P, Bugalho MJ. Disfunção tireóidea induzida pela amiodarona. Rev Port Endocrino, Diabetes e Metabolismo. 2011; 2: 31-41.
- Ramos-Dias J, Senger M. Tireóide e amiodarona: “A vítima e seu algoz” Implicações do antiarrítmico nas disfunções tireoidianas. Revista da Faculdade de Ciências Médicas de Sorocaba. ISSN eletrônico 1984-4840, Local de publicação (editar no plugin de tradução o arquivo da citação ABNT), 13, mar. 2011. Disponível em:
- Basaria S, Cooper DS. Amiodarone and the thyroid. Am J Med, 2005; 118(7): 706-14.
- Nademanee K, Singh BN, Callahan B, Hendrickson JA, Hershman JM. Amiodarone, thyroid hormone indexes, and altered thyroid function: long-term serial effects in patients with cardiac arrhythmias. Am J Cardiol. 1986; 58(10): 981-6.
- Newman CM, Price A, Davies DW, Gray TA, Weetman AP. Amiodarone and the thyroid: a practical guide to the management of thyroid dysfunction induced by amiodarone therapy. Heart. 1998; 79(2): 121-7.
- Lopes ZMTC. Patologia da tireoide associada ao consumo de amiodarona. 2013. Dissertação (Mestrado em Medicina) – Faculdade de Medicina, Universidade da Beira do Interior, Covilhã, 2013. 40p.
- Martino E, Bartalena L, Bogazzi F, Braverman LE. The Effects of Amiodarone on the Thyroid. Endocr Rev. 2001; 22( 2); 240-54.
- Loh KC. Amiodarone-induced thyroid disorders: a clinical review. Postgrad Med J. 2000; 76(893): 133-40.
- Tsang W, Houlden RL. Amiodarone – induced thyrotoxicosis: a review. Can J Cardiol. 2009; 25(7); 421-4.
- Sudheer Ahamed P, Mathew A. A Case of Amiodarone-Induced Thyrotoxicosis: A diagnostic and therapeutic dilemma. Sultan Qaboos Univ Med J. 2009; 9(3): 319-23.
- Cardenas GA, Cabral JM, Leslie CA. Amiodarone induced thyrotoxicosis: diagnostic and therapeutic strategies. Clev Clinic J Med. 2003; 70(7): 624-6, 628-31.
- Lima J, Carvalho P, Molina MA, Rebelo M, Dias P, Vieira JD, et al. Disfunção tireóidea e amiodarona. Arq Bras Endocrinol Metab, 2013; 57( 1): 71-8.
- Padmanabhan H. Amiodarone and thyroid dysfunction. South Med J. 2010; 103(9): 922-30.
- Cohen-Lehman J, Dahl P, Danzi S, Klein I. Effects of amiodarone therapy on thyroid function. Nat Rev Endocrinol. 2010; 6(1): 34-41.
- Ryan LE, Braverman LE, Cooper DS, Ladenson PW, Kloos RT. Can Amiodarone be restarted after amiodarone-induced thyrotoxicosis? Thyroid. 2004; 14(2): 149-53.
Authors
Marina Barbosa Tavares1; Paula Rodrigues Villela da Motta2; Vitória Fernandes Barros3; Camila Cezana4; Larissa Borges Ferreira5; Sabrina Marini Araujo Saar6; Carmen Dolores Gonçalves Brandão7
1,2,3 Medicine student at the Escola Superior de Ciências da Santa Casa de Misericórdia de Vitória – EMESCAM.
4,5,6 Medical Doctor graduated from the Escola Superior de Ciências da Santa Casa de Misericórdia de Vitória – EMESCAM.
7 PhD of Endocrinology from the Federal University of Rio de Janeiro – UFRJ, Medical Doctor, Professor of the Escola Superior de Ciências da Santa Casa de Misericórdia de Vitória – EMESCAM.
